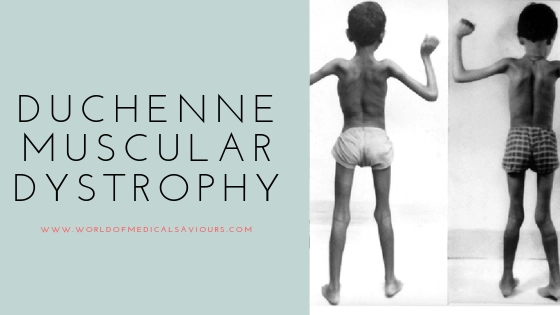
Duchenne muscular dystrophy
Duchenne muscular dystrophy is a genetic disorder characterized by advance muscle degeneration and weakness. It is one type of nine muscular dystrophies. In this disease, boys suffer and females carry the disease the only exception is Turners, where female are sufferers.
- Incidence: 1 in 3600 male births
- Defect: Mutation of the gene at Xp21 locus
- Mode of inheritance: X linked recessive trait
What causes muscular dystrophy Duchenne?
DMD is a genetic disease. Those who inherit it have a defective gene related to a muscular protein called dystrophin. This protein keeps muscle cell intact. Its absence causes rapid muscular deterioration as a child with DMD grows.
Pathogenesis
Due to the mutation of the gene on the X chromosome, there is deficient production of muscle cytoskeleton protein ‘Dystrophin’ which causes progressive weakness of muscles, particularly the proximal muscles (proximal myopathy).
Mutations in the same gene that results in partial expression of dystrophin protein produce a less severe phenotype, ‘Becker muscular dystrophy’.
Is Duchenne muscular dystrophy is painful?
Pain and sensation
The muscle deterioration is Duchenne MD isn’t usually painful in itself. Some people report muscle cramp at times; these usually can be treated with an over-the-counter pain reliever.
Clinical Manifestation
- Normal at birth or during early infancy
- Clinical manifestations usually appear by 3 years of age, e.g. frequent falls, trouble running, difficulties in climbing stairs as well as rising from floor/bed
- H/O recurrent respiratory infections
- Clinical examination shows
- Pseudohypertrophy of calves (due to hypertrophy of some muscle fibres, infiltration of muscle by fat and proliferation of collagen) Pseudohypertrophy of the calf muscle
- Wasting of thigh muscles (proximal myopathy)
- Lordotic posture
- Trendelenburg gait or hip waddle (Waddling gait)
- Presence of Gower sign, the characteristic posture
- Presence of slip through the sign (as the boy is lifted up by holding around the sides of his chest right up under his arms, the weak shoulders move upward, almost allowing him to slip through the physician’s hands)
- Presence of winging sign (winging of the scapula)
- Hypertrophy of tongue and forearm may be present but no fasciculation
- Other features
- Contractures involving ankles, knees, hips & elbows
- Scoliosis
- Cardiomyopathy, presenting as cardiac failure, persistent tachycardia, murmur Intellectual impairment
Diagnosis
Based on characteristic C/F and supports from the relevant investigations.
Investigations
- Serum CK level: Greatly elevated (15,000 – 35,000 IU/L, (normal: < 150 IU/L)
- Electromyogram (EMG): Characteristics myopathic feature but not specific for DMD
- X-Ray chest: May show evidence of pneumonia and/or cardiomyopathy (cardiomegaly)
- ECG & Fehecardiogram: Evidence of Cardiomyopathy
- Muscle biopsy shows
- Endomysial connective tissue proliferation
- Scattered degenerating and regenerating myofibrils
- Foci of mononuclear cell infiltration
- Molecular analysis has largely replaced muscle biopsy to confirm the diagnosis
Can Duchenne muscular dystrophy be cured?
There is no accepted cure for Duchenne muscular dystrophy. Treatment aims to control the symptoms to improve quality of life. Steroid drugs can slow the loss of muscle strength. They may be started when the child is diagnosed or when muscle strength begins to decline.
Treatment
Counsel parents about the nature & future of the disease.
Supportive
- Diet
- Maintain good nutrition and to prevent obesity
- Minimize osteoporosis by adequate calcium and fluoride supplementation
- Physiotherapy to delay contractures
- Prompt treatment of
- Pulmonary infections
- Cardiac decompensation (Digoxin)
- The steroid is useful in maintaining muscle strength. It does not slow the disease progression. Prednisolone, 10mg daily for 10 days of each month may be given.
- Immunization against influenza virus, in addition to other routine vaccinations
What is the commonest cause of death for someone with Duchenne muscular dystrophy?
The commonest causes of death for someone is heart failure from cardiomyopathy. Some patient is found to have genetic abnormalities of the dystrophin gene, but clinically, have symptoms between those DMD or BMD.
Prognosis
The relentless progression of weakness continues into the 2nd decade. Most patients continue to walk with increasing difficulty until 10 years of age and some are wheelchair-bound by 7 years.
Death occurs usually around 18-20 yrs of age. The common causes of death are respiratory failure, intractable heart failure, pneumonia or occasionally aspiration and airway obstruction.