7 Cervical Vertebrae: Anatomy and Important Clinical Conditions

The cervical vertebrae are the neck’s bones and comprise seven cervical (neck) vertebrae, numbered from C1 to C7 in order of increasing size.
The first four cervical vertebrae form a part of the atlas or axis bone located just below the skull. The last three cervical vertebrae make up the rest of the spine. The uppermost two cervical vertebrae articulate with each other and are joined by ligaments and muscles. They also have an intervertebral disc between them. These two bones are called the atlas and axis. The next five cervical vertebrae are fused into one bone called the body of the cervical vertebrae.
This single bone makes up most of the length of the spinal column. It has a large opening on its front side for receiving nerve roots. The lower end of this bone articulates with the dens of the skull. The two lowest cervical vertebrae are called the seventh cervical vertebrae. These two bones are not connected to any other bones. The bones enclosing the skull are called cranial bones.
Types of 7 cervical vertebrae
1. C1
This is the smallest cervical vertebrae, and it lies directly above the atlas. The atlas forms the top portion of the skull. At birth, the first cervical vertebrae are fully formed, but it does not fuse with the second cervical vertebrae until about age 15 years.
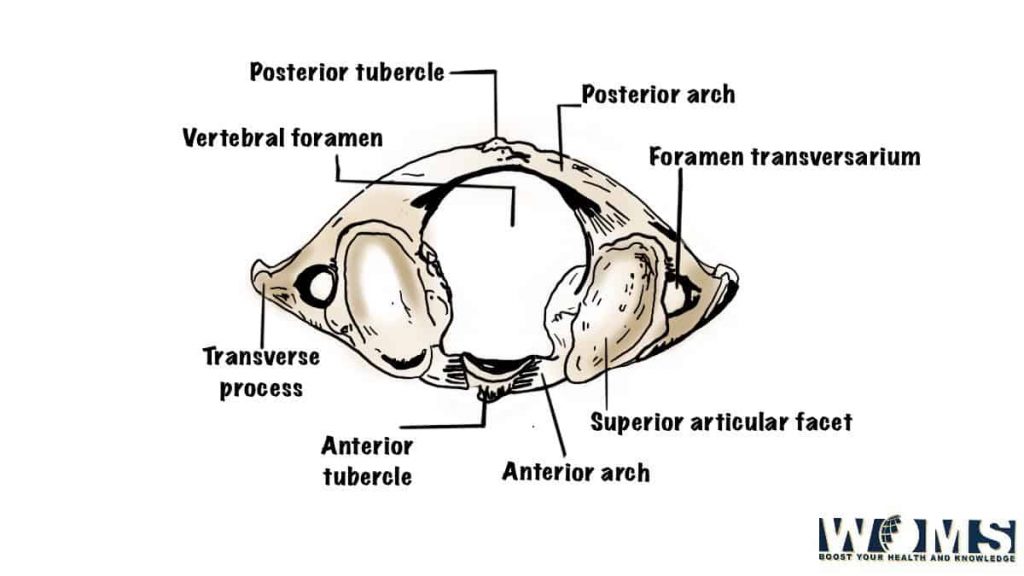
Description: It consists of a pair of arches, each arch divided into two parts. The anterior arch bears the articular processes, and the posterior arch carries the spinous process. Each arch is separated by a bony ring called the transverse process. The superior surface of the transverse process presents a concave facet for articulation with the articular surfaces of the atlas.
Clinical Relation: A fracture of the first cervical vertebra can cause severe damage to the brain stem and the spinal cord. A fracture of the dens of the skull may be associated with fractures of the first cervical vertebras.
Cause: Fractures of the dens of the head occur when there is a direct blow to the back of the neck. Injuries to the neck can result from automobile accidents, falls, sports injuries, etc.
Symptoms: Pain in the neck radiates down the arms and shoulders. There may be numbness and tingling in the hands and feet. If the injury involves the spinal cord, weakness and paralysis of the limbs may develop.
Diagnosis: X-ray examination will show if there is a fracture of the dens of the skull. CT scan or MRI will reveal more details.
Treatment: Immobilization of the neck is usually recommended if there is no neurological deficit. Surgery is indicated only if there is instability of the neck.
Prevention: The best way to prevent such injuries is to wear a helmet while riding a bicycle or motorcycle.
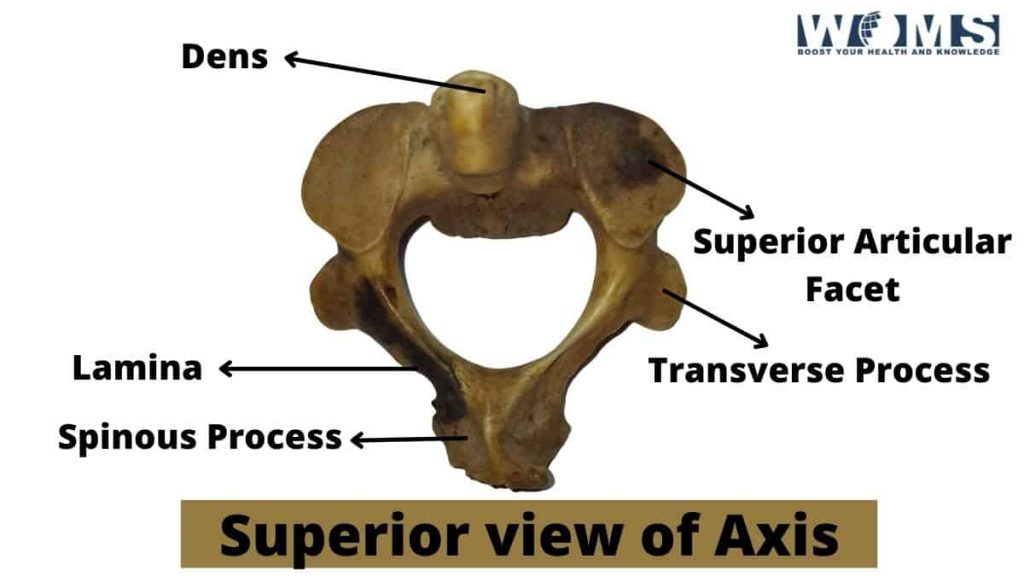
2. C2
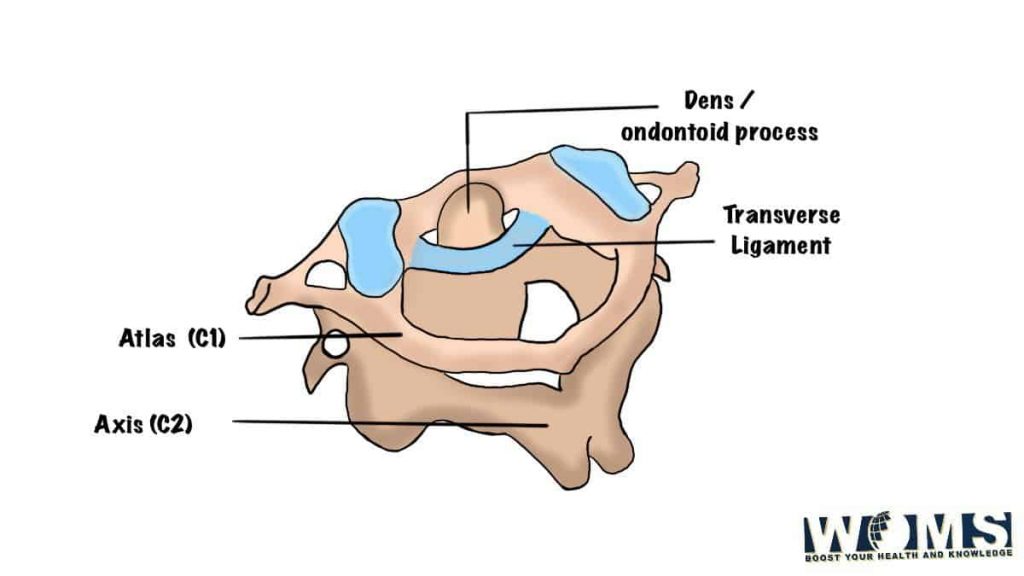
This is the second cervical vertebra. It is shaped like a wedge and lies immediately beneath the occipital bone. It is attached to the atlas through a joint called the atlantoaxial joint. The atlantoaxial joints allow rotation of the head relative to the neck. The atlantal articulation allows movement of the head in all directions except backward.
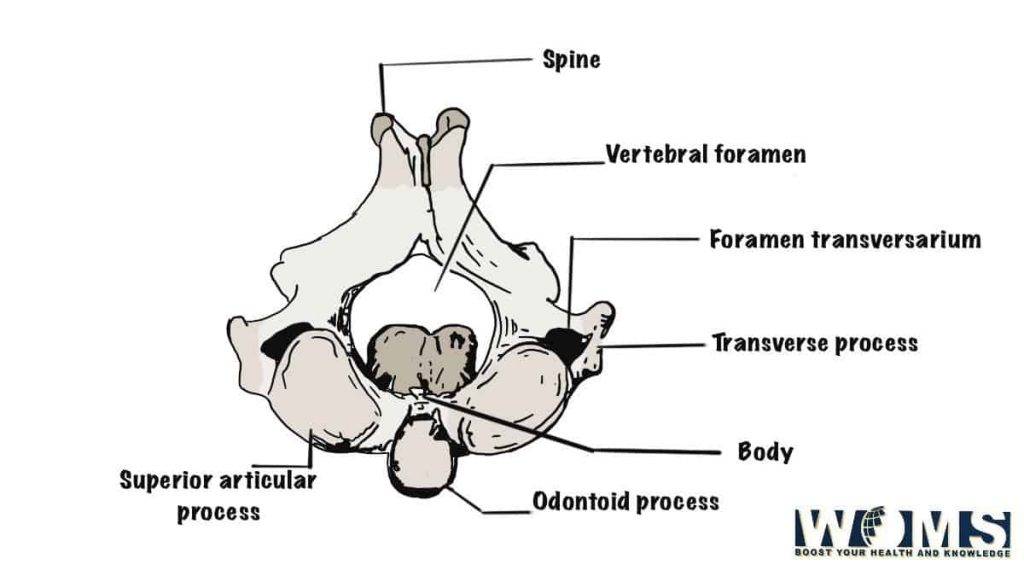
Description: The shape of the second cervical vertebra resembles a wedge. It is wider than long and has a broad base. On its lateral aspect, it is covered by a thick layer of cartilage. Its inferior surface is smooth and convex. It bears the odontoid process, which projects forward and upward. The odontoid process is a rough knoblike projection situated on the inferior articular surface of the dens of the axis.
Clinical Relation: Injury to this area causes compression of the medulla oblongata and upper part of the spinal cord. Symptoms include pain in the neck, shoulder girdle, and arm. Paralysis of the face and tongue is common.
Cause: Direct trauma to the neck or whiplash injury from an accident involving rapid acceleration/deceleration of the head can injure the atlantoaxial joint.
Symptoms: There may be an immediate onset of symptoms, including neck pain, stiffness, and inability to turn the head. This may progress over several days to weeks to involve the entire neck and shoulder girdle. Neck pain radiating to the shoulder and arm may also be present.
Diagnosis: X-rays are used to confirm the diagnosis.
Treatment: Immobilization of the neck is required.
Prevention: Wearing a helmet while riding a bike or motorcycle reduces the risk of injury.
3. C3
The third cervical vertebra (occiput) is located at the skull and spine junction. It is the smallest and most mobile of the seven cervical vertebrae. It is triangular and is covered by a thin layer of hyaline cartilage. It bears the spinous processes of the first six cervical vertebrae.
Description: It is small and triangular with three projections. It is broader than high and widest near the middle. The superior articular facet for the transverse process of the atlas faces laterally. The inferior articular facet for the spinous process of the atlas is concave.
Clinical Relation: Let’s have a look into the clinical relation of third cervical vertebrae. Trauma to this region can cause damage to the brainstem. Injury to the nerve roots that supply the arms and legs results in weakness and paralysis.
Cause: A blow to the back of the head can result in fractures of the occiput. Injuries resulting from motor vehicle accidents often occur when the head strikes the windshield or side window of the vehicle.
Symptoms: Headache, dizziness, nausea and vomiting, loss of consciousness, etc may develop following injury to the occiput.
Diagnosis: CT scan is useful in diagnosing injuries to the occiput and surrounding structures.
Treatment: Treatment includes immobilizing the head and preventing further injury.
Prevention: Using seat belts and helmets reduces the risk of injury. If possible, avoid driving after drinking alcohol.
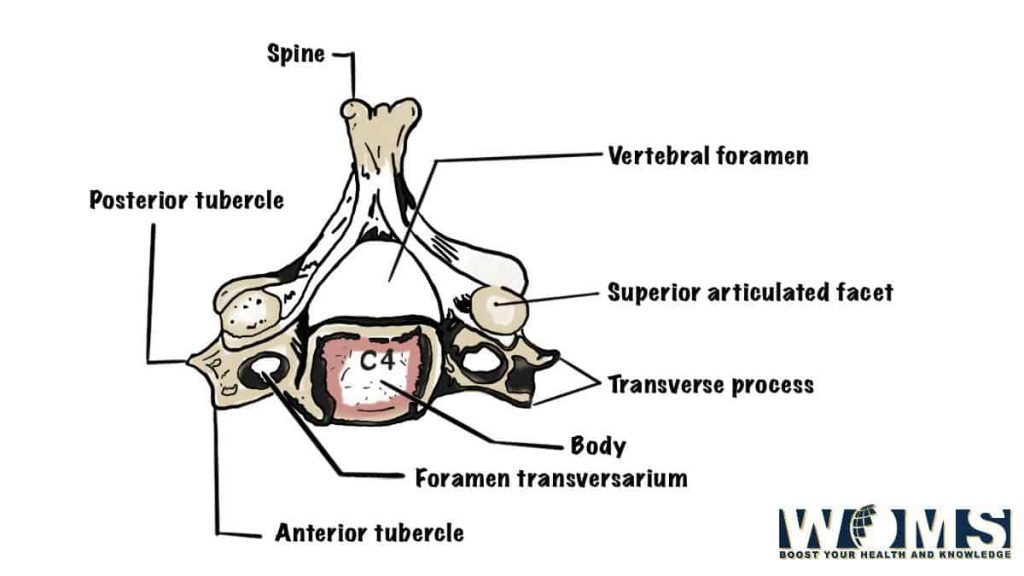
4. C4
The fourth cervical vertebra (atlas) articulates with the fifth vertebra (axis). It is the largest of the seven cervical vertebral bodies. It is shaped like a saddle and is covered by a thick membrane of fibrocartilage. It bears two large facets for each bone. One facet faces posteriorly and one anteriorly.
Description: Atlas has four processes; two lateral and two medial. Atlas is wider than tall. Lateral processes extend backward and upward from the body of the atlas. Medial processes extend forward and downward from the body of the axis.
Clinical Relation: Injury to the atlas can lead to spinal cord compression. Symptoms include headache, numbness, tingling, and weakness of the limbs.
Cause: Direct trauma to the neck or direct impact on the head can injure the atlas. Accidents involving motor vehicles usually occur when the head impacts the windshield or side windows of the vehicle.
Symptoms: Pain and tenderness along the course of the carotid artery and weakness and numbness in the extremities are common symptoms.
Diagnosis: Diagnostic tests such as X-ray, CT Scan, MRI, and angiography may be used to diagnose injuries to the atlas.
Treatment: Treatment involves immobilization of the neck and prevention of further injury. Surgery is required if there is significant displacement of the atlas.
Prevention: The use of seat belts and helmets reduces the risk of injury. Avoid driving after drinking alcohol. Wear protective gear while working around machinery.
5. C5
The fifth cervical vertebra (coccyx) articulates with the sixth vertebra (axis), forming the sacrum. It is shaped like an inverted triangle and is covered by a thin layer of hyaline cartilage. It bears two facets for each bone. A large facet faces dorsally and a smaller facet ventrally.
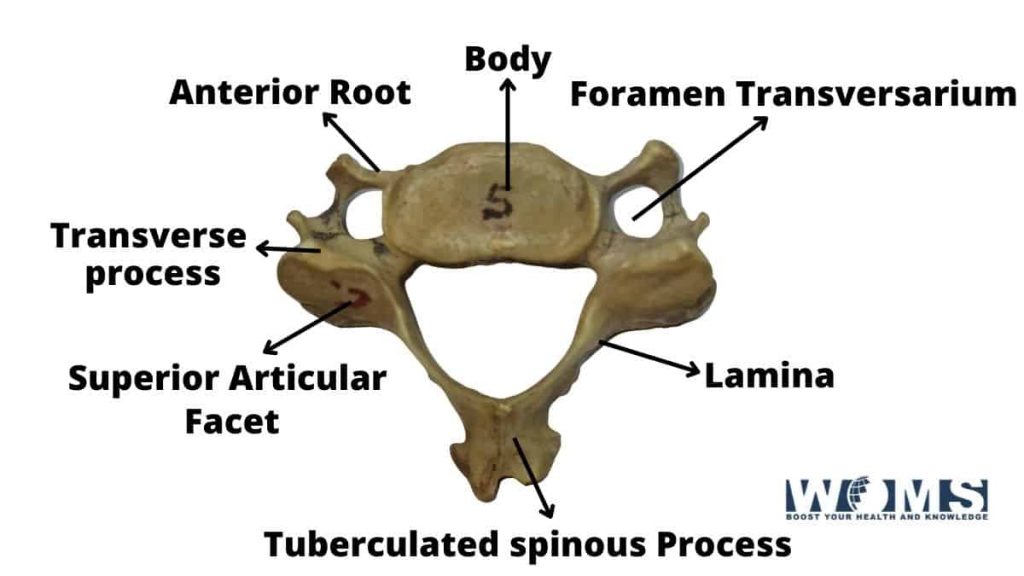
Description: The coccyx is triangular. The dorsal surface is concave, and the ventral surface is convex. The ventral process extends laterally.
Clinical Relation: Coccydynia is a pain in the coccyx caused by inflammation of the bursa sacs surrounding it. This condition is most commonly seen in athletes who overuse their muscles.
Causes: Trauma to the back of the neck causes pressure on the nerve roots leading to irritation of the nerves that supply the coccyx. Injuries due to sports activities are also a common cause of clinical conditions of these cervical vertebrae.
Symptoms: Pain radiating down the buttocks and into the legs is characteristic of this condition. The pain is often worse during exercise.
Diagnosis: X-rays show abnormalities of the coccygeal joint. An ultrasound examination may help identify soft tissue swelling.
Treatment: Treatment includes rest, anti-inflammatory medication, physical therapy, and steroid injections. Surgical removal of the inflamed area is sometimes necessary.
Prevention: Avoid repetitive lifting of heavy objects. Do not sit cross-legged. Use proper lifting techniques.
6. C6
The sixth cervical vertebra (cuboid) articulates with the seventh vertebra (axis) to form the sacrum. It has three articular surfaces; dorsal, ventral, and posterior. The cuboid is broader than long and is covered by hyaline cartilage.
Description: A cuboid is broad and flat. Its anterior border is marked by a ridge extending from the posterolateral corner to the midline. Posteriorly, it is marked by a shallow groove. On its medial aspect, it is marked by another shallow groove.
Clinical Relations: Cuboid forms part of the lateral wall of the spinal canal.
Causes: Cuboid fractures are rare because they are rarely associated with other skeletal injuries. They are more common in children than adults. Traumatic injuries are more likely to cause fractures than degenerative changes.
Symptoms: Pain in the neck or shoulder region accompanied by weakness and numbness in the arm suggest a fracture.
Diagnosis: CT scan or MRI can be used to detect fractures in this cervical vertebrae.
Treatment: Fractures involving the lateral portion of the cuboid usually heal without surgery. Fractures involving the medial portion require surgical intervention.
Prevention: No specific measures are available.
7. C7
The seventh cervical vertebra (atlas) articulates with the first thoracic vertebra (first rib). It has four articular surfaces; dorsal and ventral, right and left. The atlas is wider than high and is covered by hyaline cartilage.
Description: Atlas is wider than tall. It has a prominent transverse process that projects forward and backward.
Clinical Relations: Occasionally, the atlantoaxial joints become hypermobile and dislocate. This condition is called atlantoaxial instability. Atlantoaxial instability is very painful and may lead to neurological deficits if untreated.
Causes: Atlantoaxial instability occurs due to trauma, rheumatoid arthritis, tumors, congenital malformations, infections, etc. These are the major causes of the clinical condition of these cervical vertebrae.
Symptoms: Pain in the occiput or upper neck region along with torticollis indicates atlantoaxial dislocation.
Diagnosis: Radiographs of the skull and cervical spine help diagnose atlantoaxial dislocations. CT scans also provide good visualization of the atlantoaxial.
Treatment: Occasional cases of atlantoaxial dislocations can be treated conservatively. However, most cases need surgical treatment. Surgery involves immobilizing the head for several weeks, followed by fusion of the atlas to the axis.
Prevention: Avoid activities that involve hyperextension of the head.
Conclusion
To conclude, the cervical vertebrae are a group of jointed, bony, cartilaginous, or ossified processes that form the columns of the neck. They articulate with each other and with the head and upper torso. The human neck contains 7 cervical vertebrae and 7 thoracic vertebrae in addition to 13 pairs of ribs.
FAQs
What is the difference between an odontoid peg and dens?
Dens is a small projection on the most caudal end of the dens, which attaches the dens to the fifth cervical vertebra. Dens may be prominent or absent.
An Odontoid peg is a small peg-like structure projecting from the dens, which attaches it to the second thoracic vertebra and is also known as an odontoid process. It’s more visible than dens but may be absent as well. In some cases, both are present.
How does one distinguish a fracture of the dens from a fracture of the lamina?
A fracture of the dens is characterized by the displacement of the bone fragments into the spinal canal. A crack characterizes a lamina fracture through the entire thickness of the bone.
What is the significance of the term “atlanto-occipital” joint?
The atlantooccipital joint is the articulation between the atlas (first cervical vertebra) and the skull’s occipital bone. The atlantooccipital joint allows a small amount of head rotation around its longitudinal axis.