The Occipital bone
Occipital bone forms the region of the occiput(back of the head) and is trapezoid in shape. It presents a concavity in front and convexity behind. It encloses a large oval opening, the foramen magnum, through which the cranial cavity communicates with the vertebral canal.
Parts of occipital bone:
- Squamous part: Expanded part above and behind foramen magnum.
- Basilar part: Quadrilateral thick part in front of the foramen magnum.
- Condylar parts: Lateral parts lying horizontally, one on each side of foramen magnum bearing the occipital condyles.
Anatomical position
- Occipital condyles face downwards.
- The basilar part is directed forward and upwards.
Squamous part
Possesses:
- 2 Surfaces: External and Internal.
- 3 Angles: One Superior and two Lateral.
- 4 Borders: 2 Lambdoid and 2 mastoids, one of each on either side of the median plane.
Surfaces
- External surface: convex in all directions.
Presents:
- External occipital protuberance: a prominence midway between the posterior margin of the foramen magnum and the superior angle of the bone.
Importance:
- forms an important bony landmark and is easy. The most prominent central point of this is known as inion.
- opposite this level, the superior sagittal sinus ends and transverse sinus begins.
- gives attachment to the highest point of the ligamentum nuchae.
- Highest nuchal line: a curved line running laterally on each side from the external occipital protuberance; not well marked, often absent; gives attachment to the galea aponeurotica (epicranial aponeurosis); the area above this line is covered with the occipital belly of the occipito frontalis and the galea aponeurotica.
- Superior nuchal line: another curved line just below the highest nuchal line; well marked; its medial part gives origin to the highest fibres of the Trapezius and its lateral part to the Occipital belly of the Occipito-frontalis, below which are insertions of sternocleidomastoid and Splentus capilis. Middle third of the Line forms the apex of the posterior triangle and is related to the occipital artery.
- External occipital crest: a ridge running in the median plane from the external occipital protuberance to foramen magnum, gives attachment to the ligamentum nuchae.
- Inferior nuchal line: a curved line running laterally on
each side from the middle of the external occipital crest; gives attachment medially to the Rectus capitis posterior minor
Attachment of muscle on external surface
Insertions of:
- Semispinalis capitis : medial part of the area between superior and inferior nuchal lines.
- Obliquus capitis superior: lateral part of the area between superior and inferior nuchal lines.
- Rectus capitis posterior minor: medial part of the inferior nuchal line and into the area between the line and foramen magnum.
- Rectus capitis posterior major: lateral part of the inferior nuchal line and the area just below this line
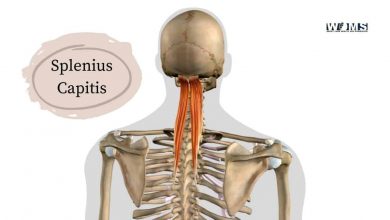
- Splenius capitis: the rough area just below lateral 1/3rd of superior nuchal line.
- Sternocleidomastoid: lateral half of the superior nuchal line.
Origins of:
- Trapezius: medial 1/3rd of superior nuchal line and external occipital protuberance.
- Occipital belly of Occipito-frontalis : lateral 2/3rd of superior nuchal line.
- Internal (cerebral) surface: Deeply concave.
Presents:
- Internal occipital protuberance: an irregular elevation in the centre opposite the external occipital protuberance.
- Sagittal sulcus: a wide groove with raised margins extending upwards from internal occipital protuberance to the superior angle. It lodges terminal part of the superior sagittal sinus and its margins give attachment to the posterior part of the falx cerebri
- Transverse sulçus : a transverse groove extending laterally on each side from internal occipital protuberance; it lodges transverse sinus; its margins give attachment to the tentorium cerebelli; the right sulcus is usually larger than the left as it is usually continuous with the sagittal sulcus; the site of confluence marked by a wide depression; the straight sinus and the occipital sinus also end at this site.
- Internal occipital crest: a prominent ridge running downwards and frontwards from internal occipital protuberance to the foramen magnum; it divides in the lower part and gives attachment to the flax cerebella; occipital sinus lies in the attached margin of the flax cerebelli.
- Fossae: the internal occipital protuberance, the sulcus for superior sagittal sinus, the sulci for transverse sinuses and the internal occipital crest divide the internal surface into 2 upper and 2 lower fossae :
- Upper fossae: triangular in shape: lodge occipital lobes of the cerebrum with meninges.
- Lower fossae: quadrilateral in shape; lodge the cerebellar hemispheres.
- Vermian fossa: a small depression at the lower part of the internal occipital crest; over it lies the inferior vermis of the cerebellum.
(ii) Angles
- Superior angle: formed by the meeting of two lambdoid borders: articulates with occipital angles of the parietal bones; corresponds with lambda (the site of posterior fontanelle in the foetal skull).
- Lateral angles: formed on each side by the meeting of the lambdoid and mastoid borders; lies in the interval between parietal bone and the mastoid part of temporal bone; corresponds with the point,
(iii) Borders
- Lambdoid borders: one on each side; extends from the superior angle to the lateral angle; articulates with the occipital border of the parietal bone of its own side to form the lambdoid suture.
- Mastoid borders: one on each side; extends from the lateral angle to the Jugular process, articulates with the mastoid part of the temporal bone.
BASILAR PART
It is a thick part, quadrilateral in shape and extends upward and forward from the foramen magnum.
Basilar part of occipital bone has two Lateral borders: one on either side; articulates with the petrous part of the temporal bone.
CONDYLAR PARTS
Lie one on each side of the foramen magnum, and connect the basilar part with the squamous part.
Possesses: 2 Surfaces:
- Superior and,
- Inferior.
Inferior Surface:
Presents :
- Occipital condyles: are two, one on each side, oval on kidney-shaped convex articular surfaces with the long axis directed forward and medially; each articulates with the superior concave articular facet of the atlas forming an atlantooccipital joint. The margins of the condyle give attachment to capsular Ligament of atlantooccipital joint; on the medial side of the condyle, a rough area or tubercle gives attachment to the alar ligament.
- Hypoglossal canal: lies above the anterior part of each condyle and below the jugular tubercle;
Transmits :
- hypoglossal nerve.
- meningeal branch of the ascending pharyngeal artery.
- emissary vein connecting basilar venous plexus with the pterygoid venous plexus.
- Condylar Fassa: a depression behind each condyle; lodges the posterior part of the superior facet of the atlas when the head is bent backwards.
- Condylar canal: occasionally present when the condylar fossa is perforated; when present,
Transmits: an emissary vein connecting sigmoid sinus with veins of the suboccipital triangle.
- Jugular process: a quadrilateral piece of bone extending laterally from the posterior half of each occipital condyle;
Presents ;
- Upper or superior surface: it is grooved to lodge the terminal part of sigmoid sinus
- lower or inferior surface; gives insertion to the Rectus capitis leteralis; there may be a small eminence termed paramastoid process in a certain percentage of skull may be long enough to articulate with the transverse process of the atlas.
- anterior surface: indented to form jugular notch; when articulated with the petrous part of the temporal bone, the jugular notch is converted into the jugular foramen.
The jugular foramen is divided into 3 compartments by two bony spicules (intrajugular processes) which
Transmits:
- Anterior compartment: inferior petrosal sinus.
- Middle compartment:
- IX (Glossopharyngeal), X (vagus) and Xl (Accessory) cranial nerves.
- a meningeal arm of the ascending pharyngeal artery.
- emissary vein may also pass.
- Posterior booth: sigmoid sinus.
Superior surface :
Presents :
Jugular tubercle (Tuberculum jugular) : an oval eminence overlying the hypoglossal canal; its posterior part presents a shallow groove for the passage of the glossopharyngeal, vagus and accessory cranial nerves to thc jugular foramen.
Foramen Magnum
It is the largest of the cranial foramina and is thus called Foramen magnum (GK Magnus-very large). Its boundary is formed by all the three parts of the occipital bone. the basilar part in front, the squamous part behind and the condylar part on either side. It is oval in shape, wider behind than in front and its longest diameter passes anteroposteriorly in the median plane. Through this foramen, the cranial cavity communicates with the vertebral canal.
It is divided into 2 compartments by the alar ligament attached to the tubercle on the medial aspect of the of the occipital condyle.
- Smaller anterior compartment transmits :
- apical ligament.
- The upper band of the cruciate ligament.
- Membrane tectoria.
- Larger posterior compartment transmits:
- The lower end of medulla oblongata with its meanings.
- Right and left vertebral arteries- ascending.
- Anterior and posterior spinal arteries- descending.
- The spinal root of accessory nerve-going above.
- Sympathetic plexus of nerves passing along the vertebral arteries and coming from the inferior cervical ganglion.
- Veins joining the venous plexus of medulla oblongata downward with vertebral plexus of veins.
- The lower part of tonsil of the cerebellum may also project on each side of the medulla oblongata.
The anterior margin of the foramen gives attachment to the anterior atlantooccipital membrane while the posterior margin to the posterior atlantooccipital membrane.
Clinical significance
Trauma to occiput can cause a fracture to a base of the skull, called a basilar skull fracture. The basion-dens line as seen on the radiograph is the distance between the basion and the tops of dens, used in the diagnosis of dissociation injuries.
The identification of the location of the fetal occiput is important in delivery.