Ligament of Treitz: An In-Depth Look at Its Anatomical Significance
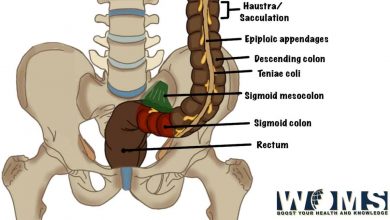
In medical terminology, the ligament of Treitz is referred to as duodenojejunal flexure. It is considered a tissue band in the abdomen. Different anatomists describe the ligament of Treitz as a suspensory muscle of the duodenum. Moreover, it arises from the connective tissue present near the stem level of celiac and superior mesenteric arteries. It terminates as a non-striated muscle into the 3rd or 4th part of the duodenum.
Considering the formal definition, ligaments in the gastrointestinal tract are the folds of the peritoneum that usually connect one viscera to the other viscera. It may connect the viscera to the adjacent abdominal wall either anterior or posterior. This article explains all the basic anatomical concepts of this ligament with a proper illustration.
Anatomy of the ligament of Treitz:
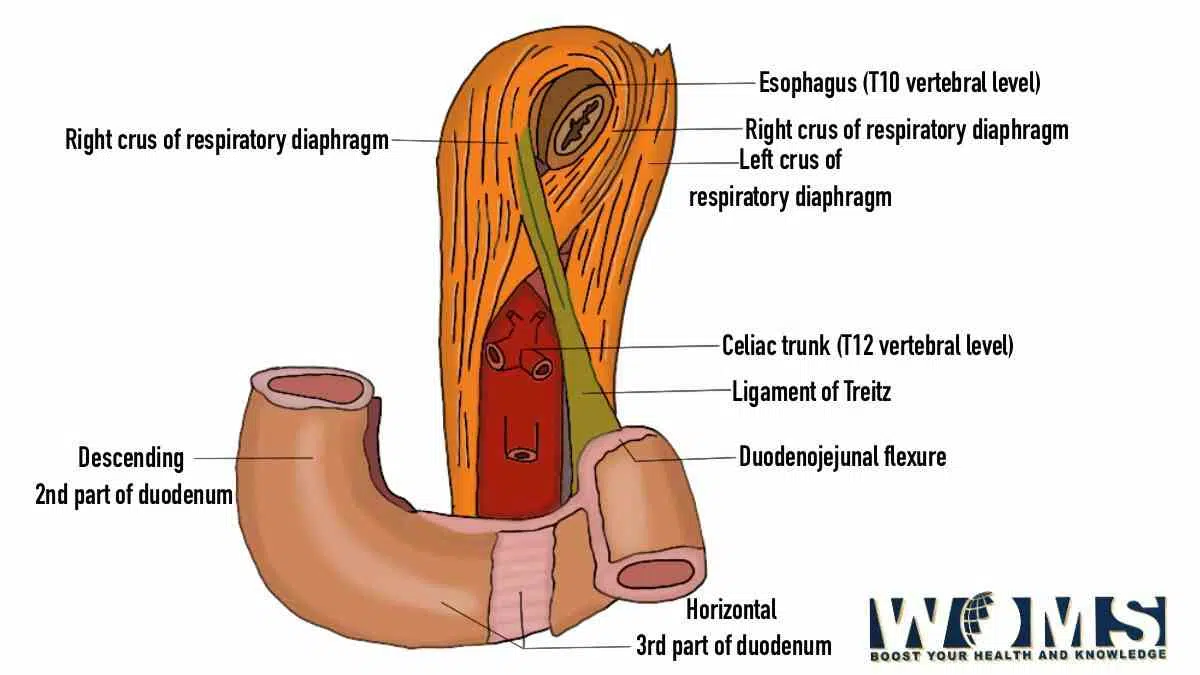
Wenzel Treitz described this ligament for the first time as a soft, triangular-shaped, and muscular band. This band extends from the superior region of the duodenojejunal junction. As it is a ligament of the abdomen, it is a double fold of the peritoneum. It lies posteriorly to the pancreas but anteriorly to the left side renal vein. In addition, the ligament lies parallel to the inferior mesenteric artery, representing an anatomical landmark.
The ligament of Treitz is formed of two parts, having communication through the connective tissue enclosing the celiac artery. Let us look at the two particular parts of the ligament of Treitz.
Superior part – This part is also known as Hilfmuskel, a german word for accessory muscle. It exhibits an elongated triangular shape being wider at its origin and narrow at its insertion point. It is a type of striated skeletal muscle. In addition, it originates from the right crus of the diaphragm near the level of esophageal hiatus. Moreover, this part is converted by the fibrous structure just before termination into the connective tissue. It twirls around the esophagus forming a loop.
Inferior part – it is also known as the suspensory muscle of the duodenum. It is a thin muscular band that originates from the celiac trunk as a band of connective tissue. Histologically, it is a band of smooth muscle. In addition, it originates from the duodenum and duodenojejunal flexure. It also exhibits a triangular shape at its origin point. But it tapers down towards its point of fibrous insertion.
Considering both parts of the ligament, modern anatomy experts accept that the ligament is a mixed muscle with different parts being absent or rudimentary.
Function of the ligament of Treitz:
The ligament of Treitz is a combination of smooth and skeletal muscle. So different anatomists hypothesize different functions according to the nature of the ligament. It should provide proper stability to the duodenojejunal flexure and prevent it from being displaced. But, because of its thin nature, it is unable to provide the main function of stability. These are some of the main functions of the ligament.
- It provides a contraction force to move the contents of the intestine along the tract.
- It provides a little bit of support to anchor the duodenum.
- The connection of the ligament to the 3rd and 4th part of the duodenum provides an inlet near the duodenojejunal flexure. In this way, it helps in the complete emptying of the bowel.
- It is an important anatomical landmark for surgeons.
- It is a defining point between the upper and lower gastrointestinal tract. It offers great help to differentiate between upper and lower gastrointestinal bleeding. Bleeding of the gastrointestinal tract above the surface of the ligament is referred to as upper GIT bleeding. Whereas bleeding below the surface of the ligament is known as lower GIT bleeding.
You may also be interested to read this detailed article on the anatomy of stomach.
Clinical importance of the Ligament of Treitz:
This ligament is an important anatomical structure for the anatomist and surgeons. It serves as a landmark to denote the duodenojejunal junction. It also highlights the point from where the small intestine moves from the retroperitoneal duodenum to the intraperitoneal jejunum. Surgeons understand the importance of this ligament during surgical procedures for anastomosis by measuring the jejunum.
Embryological importance of the ligament of Treitz:
This ligament performs a main role during the developmental phases. Considering embryological facts, the suspensory muscle of the duodenum is produced from the mesoderm, a germ layer. As the suspensory muscle of the duodenum, it offers the main role during the embryological rotation of the small intestine. This rotation depicts itself as the superior retention bend.
Anatomical variations of the ligament of Treitz:
The ligament of Treitz exhibits multiple anatomical variations in terms of attachment point and length. Despite its classical appearance, this ligament is attached to the duodenojejunal flexure only in 0 to 8% of the population. In contrast, about 40 to 60% time, it is attached additionally to the 3rd and 4th parts of the duodenum. Whereas, in 20 to 30%, it shows only attachment to the 3rd and 4th part of the duodenum. Attachment in a separate division to the duodenum is quite unusual.
Innervation:
The ligament of Treitz received its nerve supply from the non-myelinated nerve fibers from the mesenteric and celiac plexuses.
Clinical conditions associated with the ligament of Treitz:
There are several abnormalities associated with the ligament of Treitz resulting in the abnormal involvement of other structures. The ligament of Treitz has the main function during the developmental phases of the gut. Let us have a look at the medical conditions involving the ligament of Treitz and associated structures.
Intestinal malrotation:
It is a congenital problem due to pathologic rotation or peritoneal fixation during developmental phases. Any pathologic increased length of the ligament of Treitz may induce intestinal malrotation. This condition results in the abnormal orientation of the duodenojejunal junction and multiple large or small loops in the peritoneal cavity. Intestinal malrotation usually involves the midgut. Intestinal malrotation exhibits itself during the starting months of life as acute abdominal symptoms. Sometimes, intestinal malrotation remains dormant. Whereas, on the other hand, it represents intermittent, vague abdominal symptoms. Intestinal malrotation is also in patients with syndromes.
Superior mesenteric artery syndrome:
Abnormal thickening, shortened length, or hypertrophy of the ligament of Treitz may lead to superior mesenteric artery syndrome. It may also indicate proximal intestinal obstruction. There are several causes including cachexia, weight loss, external compression, severe immunocompromised conditions, or lumbar lordosis. A short and hypertrophied ligament of Treitz may be an uncommon cause for superior mesenteric artery syndrome. It typically manifests itself as nausea, anorexia, a feeling of fullness, or partial relief on postural changes( prone positioning).
Gastrointestinal bleeding:
Most of the patients commonly present with gastrointestinal bleeding. It is also associated with increased mortality rates. The ligament of Treitz serves as an anatomical landmark for clinicians to differentiate between the upper and lower GIT bleeding. Peptic ulcers are the leading reason for upper GIT bleeding. Whereas, diverticulitis is the main reason for lower GIT bleeding.
Neoplasm related to the ligament of Treitz:
Primary malignancies are 1-2% of gastrointestinal tumors. There may be metastatic deposits available in the ligament of Treitz indicating secondary tumors. Moreover, metastatic deposits are common to involve the ligament of Treitz as compared to the primary neoplasms. These Mets can spread from the surrounding organs like the stomach, ovary, or colon. Patients with neoplasms present with vague symptoms involving pain, anemia, or GIT bleeding. These lesions are usually diagnosed during the treatment of any other pathology causing the problem.
Conclusion:
Ligament of Treitz is a fibro-muscular band present at the duodenojejunal flexure. It consists of two muscular parts with proper differentiation. In addition, it is a differentiating point between the foregut and midgut. It provides a little bit of support to the duodenum due to its muscular nature. Moreover, it also helps to move the bowel content along the GI tract. Anatomists and surgeons use this as a reference point during surgical procedures.
Problems involving the ligament of Treitz are usually congenital. It may arise several problems during the developmental phases. As the suspensory muscle of the duodenum helps in the rotation of the small intestine, any defect in the ligament of Treitz may cause intestinal malrotation.
Frequently asked questions (FAQs)
What is the prominent thing that separates the upper GI tract from the lower GI tract?
There is an exact demarcating point that serves the upper GI tract from the lower GI tract. The suspensory muscle of the duodenum serves as a differentiating point between the foregut and midgut. Clinicians also use this point to differentiate upper GIT bleeding from lower GIT bleeding.
When should we contact the physician regarding the intestinal problems?
Usually, problems associated with the ligament of Treitz are congenital. If you find any one of the following signs and symptoms, consult your doctor immediately.
● Blood in stool appears as Black or red indicating lower GIT bleeding.
● Hematemesis – blood in vomiting indicates upper GIT bleeding
● Sudden weight loss or unable to gain weight
● Persistent nausea
● Constipation from several days
● Persistent pain in the stomach
● Any visible swelling in the belly region
● Continuous vomiting