A 14- year-old Boy with unidentified recurring fever

Background
A 14 years old boy in Japan presents with a 2-week history of unrelenting fever and generalized fatigue. He has had been experiencing mild headaches and associated mild neck stiffness, with an elevation of his temperature that resolves with antipyretics. He and his family have visited several community emergency departments, where he has had multiple negative lumbar punctures and was last given a diagnosis of aseptic meningitis.
He developed dry, fissured lips and some skin peeling in the recent days. He is otherwise without any specific symptoms, such as cough, shortness of breath, abdominal pain, back pain, or urinary complaints. He has no significant medical or family history, and he is not taking any medications.
Physical Examination and Workup
On physical examination, the patients is ill appearing, fatigued, and febrile . He has a blood pressure of 125/66 mm hg , a heart rate of 116 beats/min with a regular rhythm, a respiratory rate of 19 breaths/ min, and an oxygen saturation of 96% while breathing room air. He has mild bilateral conjuctival infections with limbic sparing , enlarged right lymphadenopathy , and a mild desquamating rash between his fingers.
His lungs sounds are clear bilaterally , and cardiac auscultation reveals a normal first heart sounds and a normal physiologically split second heart sound . no murmurs, thrills, rubs, or gallops are appreciated. No significant conductions abnormalitiesare noted on ECG, but an initial transthoracic echocardiogram (TTE) i n the emergency department, although a poorly delineated study , raises suspicion for cardic motions abnormalities .
Labrotary tests are performed that reveals a markedly elevated white blood cell count of 21.6*103 cells/µL , with 15% bands; a slightly low hemoglobin level of 12.2 g/dL ;and an elevated platelates count of 720 * 103 cells/µL. Blood cultures are obtained and sent to the lab. Intravenous immunoglobulin and antibiotics are empiracally initiated for suspicion of kawasaki diseases(KD), scarlet fever , or sepsis , and the patient is admitted for cardiac monitoring.
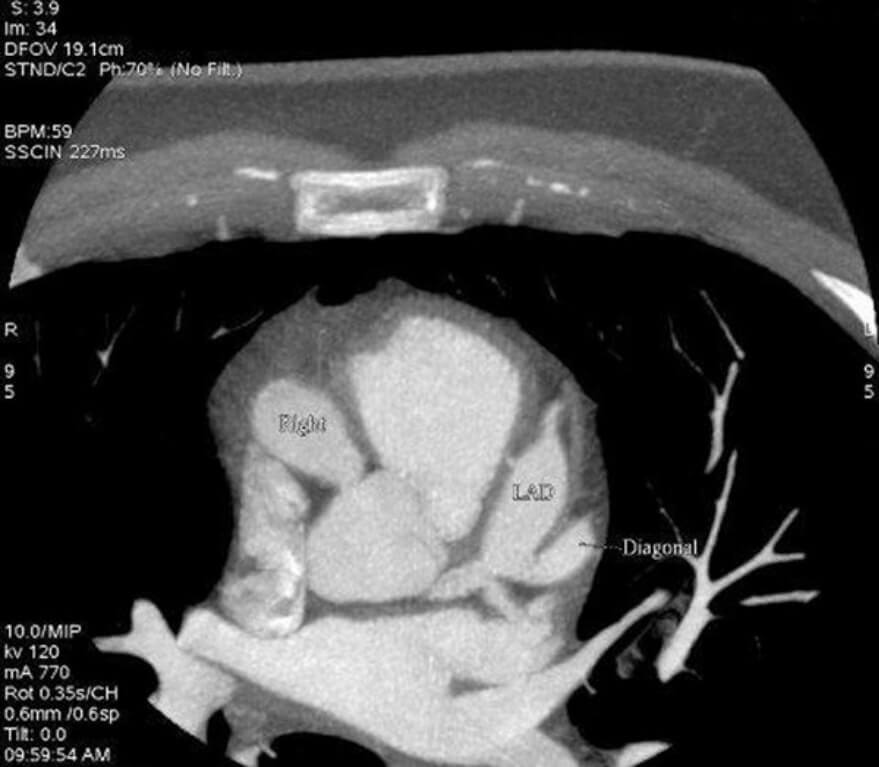
The following day, the patient is referred for coronary CT angiography (CCTA) for better delineation of the cardiac and coronary anatomy. Images are obtained using low dose protocols, with an estimated radiation dose of 5 mSv (figure 1) of