Ligaments of Shoulder Joint
The shoulder joint is also known as the glenohumeral joint. This shoulder joint exhibits the specifications of a synovial joint. It is a ball and socket-type joint that maintains the connection between the upper limb and the axial skeleton. This joint is between the articulating surface of the glenoid fossa of the scapula and the humeral head. Moreover, there are also several ligaments of the shoulder joint that offer maximum security of movement.
Functionally, this shoulder joint is a diarthrodial, multiaxial joint. It is one of the main articulations of the pectoral girdle. In addition, the shoulder joint exhibits a greater extent of mobility as compared to the other joints of the body. There are several stabilizing structures around the shoulder joint that provide greater degrees of motion in several planes.
This article summarizes the best details about the movements, anatomical features, functions, and different ligaments of the shoulder joint. Take a deep dive with us to learn and grab the optimum concepts related to the anatomy of the shoulder joint.
What are the main structures involved in the shoulder joint?
Joints are formed by the union of two articulating surfaces of different structures. Besides these articulating surfaces, these joints have several cartilages, ligaments, tendons, and fluids to maintain proper movements. Let us look at the important structures involved in the formation of a shoulder joint.
1. Articulating surfaces
Articulating surfaces are the endpoints of two bones at which joint forms. Joints help to connect these articulating surfaces. In the case of the shoulder joint, there are two articulating surfaces.
- Humeral head
- The glenoid cavity of the scapula
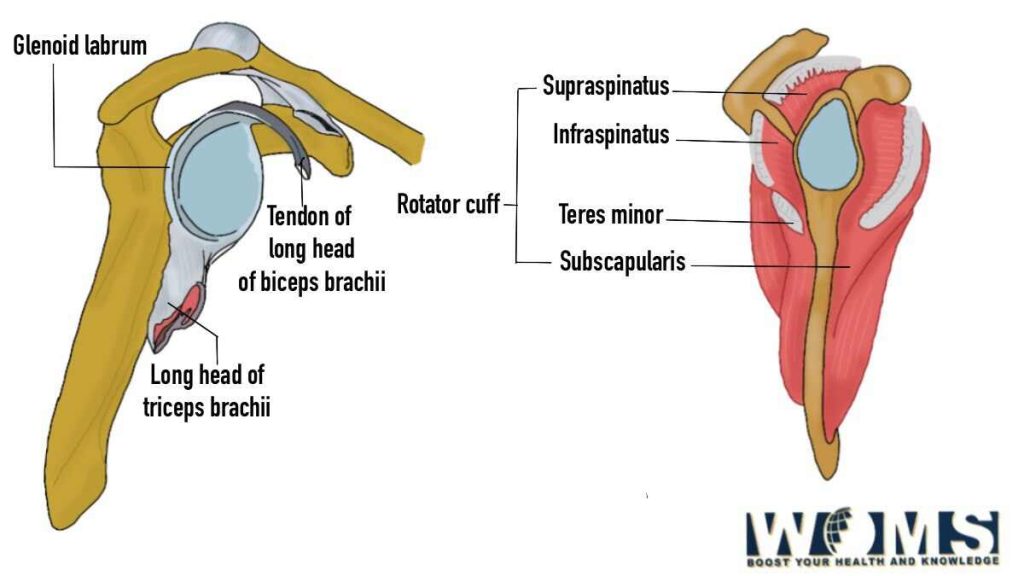
A shoulder joint is a form of synovial joint. Therefore, both of these articulating surfaces are properly coated with hyaline cartilage. The glenoid cavity is of pear-shaped depression from the superolateral aspect of the scapula. The glenoid labrum is connected to the margins of the glenoid cavity. It helps to deepen the concavity of the glenoid fossa. The humeral head is convex and quite larger than the glenoid cavity. Therefore, only one-third of the humeral head maintains contact with the glenoid labrum and cavity.
This type of bony anatomy offers a greater extent of movement at the shoulder joint. But, this increased range of movement decreases joint stability. Moreover, it also makes this shoulder joint more prone to injury.
2. Joint capsule
The joint capsule is completely enclosed by a fibrous sheath. This fibrous sheath extends from the marginal border of the glenoid fossa up to the neck of the humerus. In this way, it covers both the articulating surfaces. The synovial membrane lines the internal borders of the joint capsule. This synovial membrane produces the synovial fluid to decrease the frictions and lubricate the articulating surfaces.
This joint capsule is of lax type, offering greater mobility to the shoulder joint. This joint capsule has two main openings. These are as follows:
- One opening point is present between the greater and lesser tubercle of the humerus bone. It is the opening through which the tendons for the long head of the biceps brachii moves.
- The other opening is between the superior and middle ligaments. From this point, the subscapular bursa connects with the shoulder joint cavity.
3. Synovial bursae
When two bones move over each other, there is a greater chance of increased friction. To reduce friction, there are several synovial bursae present between the articulating surfaces. These synovial bursae work as a cushion material between the contacting points of a joint. There are several synovial bursae that enclose the joint. But some of them are clinically important. These are as follows:
- Subacromial bursae – it is also known as subdeltoid bursae. This bursa is present between the deltoid muscle and joint capsule viewing from the superolateral angle of the joint. It is located deep to the deltoid and acromion but superficial to the joint capsule and supraspinatus tendon. It reduces the friction below the deltoid muscle and enhances the motion range. Moreover, it does not directly contact the shoulder joint. Any inflammation, subacromial bursitis, may cause pain in the shoulder joint.
- Subscapular bursa – This bursa lies between the subscapularis tendon and the joint capsule. It reduces the frictional damage caused by the movement at the shoulder joint. In addition, it also prevents wear and tears on the subscapularis tendon during internal rotation of the joint.
- Subcoracoid bursae – This bursa is usually located between the coracoid process and the subscapularis muscle. Just like other bursae, it also helps to reduce the frictional forces produced between the articulating surfaces.
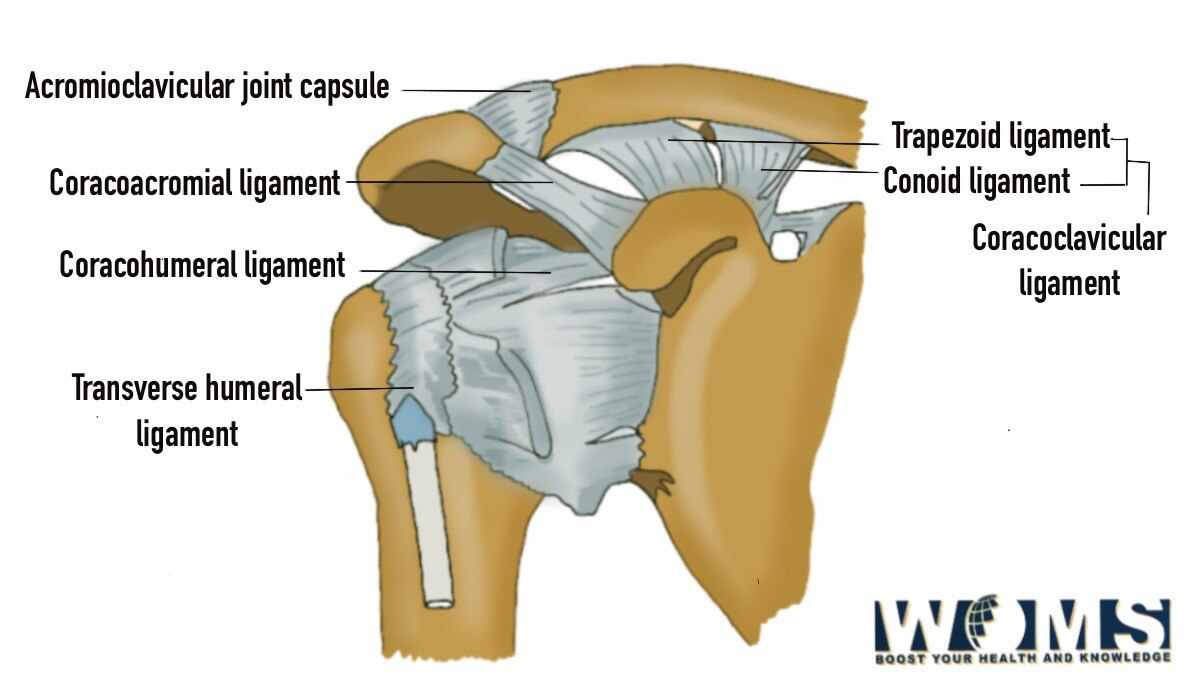
4. Ligaments of the shoulder joint
There are multiple ligaments of the shoulder joint that provide stabilizing factor. These ligaments of the shoulder joint offer a greater but secured movement over a limited range. These ligaments stabilize the bony articulating surfaces by limiting the movement of the shoulder joint. In this way, it prevents the dislocation of the head of the humerus bone beyond the glenoid cavity. Let us have a detailed look at the different ligaments of the shoulder joint to understand the basic concepts.
There are three main ligaments that surround the shoulder joint. These are as follows:
- Glenohumeral ligament
- Coracohumeral ligament
- Transverse humeral ligament
Glenohumeral ligament
It is a capsular ligament that surrounds the shoulder joint. It is composed of three types of ligaments.
- Superior glenohumeral ligament – This ligament has boundaries starting from the supraglenoid tubercle of the scapula. From this, it limits itself to the lesser tubercle of the humerus. These ligaments prevent inferior translation and external rotation of the humeral head during shoulder adduction.
- Middle glenohumeral ligament – it extends from the anterior glenoid border of the scapula to the inferior aspect of the superior glenohumeral ligament. This ligament provides a stabilizing effect to the anterior joint capsule by limiting external rotation.
- Inferior glenohumeral ligament – This ligament is like a sling present between the glenoid labrum and the inferomedial aspect of the neck of the humerus. It is the strongest glenohumeral ligament with more length and thickness. It is divided into anterior and posterior bands. Both bands offer stabilizing effects while limiting external and internal rotation.
Coracohumeral ligament:
As the name indicates, this ligament extends its boundaries from the coracoid process of the scapula to the tubercle of the humerus. This ligament of the shoulder joint is divided into anterior and posterior bands.
- Anterior aspect stabilizes the joint by limiting the extension.
- Whereas, the posterior aspect stabilizes the joint by limiting flexion.
Both anterior and posterior divisions limit the inferior and posterior translation of the head of the humerus. This ligament helps to maintain the weight of the arm at rest against gravity.
Transverse humeral ligament
This ligament extends in a horizontal direction extending in between the humerus tubercle. In addition, it covers the intertubercular cavity and the long head tendon of the biceps brachii muscle. In this way, this ligament prevents the movement of tendons from the sulcus.
What are the muscles that are associated with the shoulder joint?
Muscles act as a dynamic factor to maintain multiple movements occurring at the shoulder joint. There are several muscles associated with the shoulder joint. These are as follows:
Flexors
- Deltoid muscle (anterior part)
Extensors
- Latissimus Dorsi muscle
- Triceps brachii muscle
- Teres major muscle
- Deltoid muscle (posterior part)
Rotator Cuff
- Subscapularis muscle
- Infraspinatus muscle
- Supraspinatus muscle
- Teres minor muscle
Internal rotator
- Teres major muscle
- Latissimus Dorsi muscle
- Pectoralis major muscle
- Subscapularis muscle
External rotator
- Infraspinatus muscle
- Teres minor muscle
Adductors
- Pectoralis major muscle
Abductors
- Deltoid muscle
- Supraspinatus muscle
Blood supply of the shoulder joint
The shoulder joint receives its blood supply through the
- Anterior and posterior circumflex humeral artery
- Circumflex scapular artery
- Suprascapular arteries
Lymphatic drainage of the shoulder joint
There are several lymph nodes present in the upper extremity which are located in the axillary region.
Innervation of the shoulder joint
The shoulder joint receives its nerve supply through the subscapular nerve C5 to C6. It is a branch of the posterior cord of the brachial plexus. The joint capsule receives its nerve supply through various branches. These are as follows:
- Suprascapular nerve
- Axillary nerve
- Lateral pectoral nerve
What are different kinds of motions possible at the shoulder joint?
Joints offer a variety of motions to different extents. Let us have a look at the possible motions at the shoulder joint.
Abduction – movement in the frontal plane: It is defined as moving the upper limb away from the midline in the frontal plane. In this movement, the elevation of the humerus bone elevates the glenoid cavity in the frontal plane.
Flexion – movement in the sagittal plane: It is defined as moving the upper limb anteriorly in the sagittal plane. It offers about 180 degrees of movement. It is the forward but upward movement of the humerus bone on the glenoid cavity in the sagittal plane.
Extension – movement in the sagittal plane: It is defined as moving the upper limb posteriorly in sagittal orientation. It offers about 45 to 60 degrees of movement. It is the upward movement of the humerus towards the back side of the body on the glenoid fossa in the sagittal plane.
Internal rotation – movement in medial direction: It is defined as the rotation towards the midline in the vertical axis. It offers 70 to 90 degrees of movement. Moreover, it is the rotation of the humerus bone on the glenoid fossa in the medial orientation.
External rotation – movement in the lateral plane: It is defined as the rotation in a lateral direction in the vertical axis. In this, rotation of the humerus bone occurs in the lateral direction.
Scapular plane Abduction: In this movement, the elevation of the humerus bone occurs on the glenoid fossa in the scapular plane. The Scapular plane lies between the coronal and sagittal planes.
Horizontal adduction: In this movement, humerus bones move on the glenoid fossa medially gut with some degree of shoulder flexion.
Clinical significance of the shoulder joint
The shoulder joint is one of the most mobile joints of the body. Moreover, this shoulder joint offers a greater degree of function by performing different movements. The shoulder joint may suffer from local injuries and cause joint dysfunction. These are some of the common clinical problems associated with the shoulder joint.
Joint dislocation
A joint dislocation is a form of displacement of the bony articulating surfaces. Anterior (95%), posterior (4%), and inferior (1%) dislocations are possible according to the displacement of the humeral head.
- Tendon inflammation
- Bursitis
- Arthritis
- Impingement
- Instability
These are some of the most common problems of the shoulder joint enforcing proper examination by the doctor.
Frequently Asked Questions (FAQs)
What are the static and dynamic structures associated with the shoulder joint?
Static or stabilizing structures are usually the anatomical features of articulating surfaces, joint capsule, glenoid labrum, ligaments of the shoulder joint, and negative intra-articular pressure.
In contrast, dynamic structures are long head biceps tendon, rotator interval, rotator cuff muscle, and periscapular muscle.
Which thing holds the shoulder joint in position?
These ligaments of the shoulder joint are the main source to stabilize the joint in its position. They keep the shoulder in place and prevent dislocation.